Rhythm disturbances (general)
In simple terms, there are arrhythmias that are too slow and too fast (palpitations). A disturbance of the sinus node or AV node can slow down the heartbeat and thus cause poor performance, dizziness and, in the worst case, unconsciousness.
Rapid arrhythmias are caused, for example, by muscle cells that "become electrically active on their own" and thus cause extra beats in the heart.
Other causes of palpitations are additional conduction pathways or "short-circuit connections" in the area of the patient's own conduction system. As a patient, you often feel the rapid rhythm disturbances as palpitations/stumbling or palpitations.
Particularly rapid cardiac arrhythmias are dangerous as they can lead to unconsciousness and, in the worst case, even death. In any case, cardiac arrhythmias should be carefully examined in order to distinguish between harmless and dangerous ones and, if necessary, to start appropriate treatment.
Diagnostics of cardiac arrhythmias
Long-term ECG and event recording device (event recorder)
Rhythm disturbances are often not persistent, but occur sporadically. In order to detect them, an ECG (long-term ECG) must be recorded over a longer period of time (24-48 hours). Sometimes the arrhythmias are so infrequent that they are not necessarily recorded in the long-term ECG. In this case, a so-called event recorder helps, which is only activated when the patient feels the symptoms.
Elektrophysiologische Untersuchung (EPU)

ECG recordings from the body surface are often not sufficient for an accurate diagnosis of arrhythmia. ECGs" directly from the heart are then required. For this purpose, thin electrodes are placed in the patient's heart via the vein in the groin under sedoanalgesia and after local anaesthesia in order to record the electrical activation there directly (Fig. 1)
Catheter ablation
A particular advantage of electrophysiological examination is that many arrhythmias can be diagnosed and then treated in one session. Controllable electrodes are used for this purpose, which can be made hot (or cold) at the tip. As a result, the tissue in the heart adjacent to the tip of the electrode is cauterised (catheter ablation).
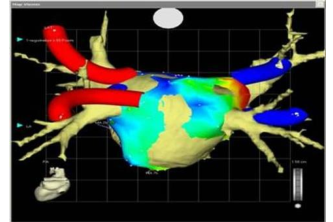
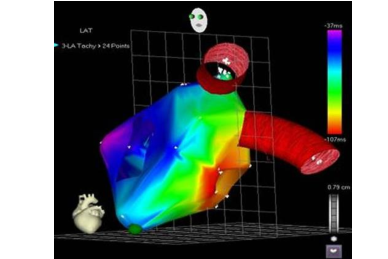
For complex arrhythmias, "electroanatomical" 3-dimensional orientation methods are used (CARTO see Fig. 2). This makes it possible to spatially visualise the spread and regression of electrical activity and thus locate and treat the arrhythmia much more precisely.
In the last 10 years, 342 children and adolescents with arrhythmias have been ablated. Complex procedures such as transseptal puncture, CARTO merge (Fig. 3) and magnetic navigation procedures have also been used.