
Ductus - Stenting
In newborns with complex heart defects (e.g. Hhypoplastic left heart, hypoplastic right heart), the ductus arteriosus is vital. This vessel can be used to maintain blood flow to the lungs as well as to the body, as the blood from the different circulatory systems mixes through it. This is also referred to as ductus-dependent heart defects.
Stent implantation in the ductus arteriosus is not yet a standard procedure. It is currently only carried out in centres with the greatest experience in cardiac catheter interventions.
The aim of ductal stenting is to keep the duct open for around 4-6 months and then perform the surgical operation. In addition to the acute treatment, the affected patients have the chance to avoid having to undergo extensive surgery with a heart-lung machine in the neonatal phase. Many experts believe that this can have a positive effect on the child's development.
Indication
Ductal stenting can be selected as an alternative to surgical interventions or in addition to surgery. The most common indications are
- As an alternative to aortopulmonary shunting
- Pulmonary valve atresia
- Pulmonary stenosis in the context of complex heart defects
- Hypoplastic right heart
- Acute treatment for ductal stenosis (heart defect not known prenatally)
- Alternative to Norwood I surgery for hypoplastic left heart
- Together with pulmonary artery banding (hybrid procedure)
- For borderline small left ventricle
- For serious non-cardiac organ malformations in addition to the heart defect
- In premature babies for whom a Norwood operation is not possible
Technics
Depending on whether the perfusion is ductus-dependent lung perfusion or ductus-dependent perfusion of the systemic circulation, the access route via the inguinal vein or inguinal artery is selected. Depending on the anatomy of the ductus, access via an artery in the arm (axillary artery) may also be helpful.
The duct is probed with a guide wire and the respective catheter with the stent is placed via this. The special feature compared to stent implantations in other vessels is that the child's life depends on the ductus arteriosus. Manipulations during implantation are therefore always a risk for an acute deterioration of the condition.
The implants are stents that are usually also used in other vessels. Depending on the different circulatory situations, the newborn requires the following stent sizes:
- Duct-dependent pulmonary circulation - stent diameter 3.5-4.5 mm
- Duct-dependent body circulation - stent diameter 6-9 mm
Both balloon-expandable and self-expanding stents are used.
Course
In most patients, the ductus stent is removed or ligated during the follow-up operation. Some patients with pulmonary atresia in whom it is possible to expand the valve (radiofrequency perforation) can leave the stent in place. It usually closes on its own after a few months. These patients can be treated by intervention alone despite a serious heart defect.
Visualisation of the ductus arteriosus in a pulmonary atresia
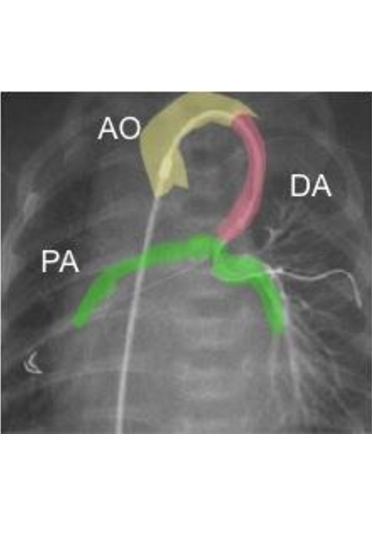
The blood flows from the aorta (yellow) via the ductus (pink) into the pulmonary artery (green). There is no pulmonary valve here and the ductus is the only blood supply for the pulmonary artery (AO = aorta, DA = ductus arteriosus, PA = pulmonary arteries).

Angiography of a severely narrowed ductus arteriosus (A) into which a stent has been inserted on a balloon catheter (B). After stent deployment, an unimpeded outflow of contrast medium from the aorta into the pulmonary artery can be seen (C).