
Atrioventricular septal defect (AVSD)
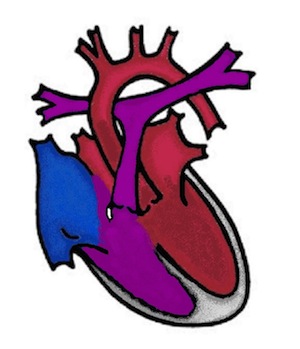
The atrioventricular septal defect (AVSD) is also known as the AV canal and is a malformation of the septum between the atria and ventricles as well as the AV valves (atrioventricular valves - valves between the atria and ventricles). All these structures are formed by the fusion of the so-called "endocardial cushions". If fusion is absent or defective, a hole is created in the lower part of the atrial septum and another hole in the upper part of the ventricular septum. Instead of two AV valves, a common AV valve with usually five leaflets is formed. This heart defect can be associated with other malformations - e.g. tetralogy of Fallot or double outlet right ventricle (DORV). Children with trisomy 21 (Down's disease) are particularly frequently affected.
What are the effects of an atrioventricular septal defect (AVSD)?
The holes in the cardiac septum lead to short-circuit connections from the left heart to the right (left-to-right shunt). There is a shunt from the left ventricle into the right ventricle as well as between the atria. The common AV valve is often leaky (AV valve insufficiency) and this contributes to further impaired cardiac function. If the proportion of the ventricular defect is very large, the pressure in the pulmonary circulation increases (pulmonary arterial hypertension).
Symptoms
The children become ill in the first few weeks of life - "heart failure" occurs. The signs that can be observed are shortness of breath, heavy sweating, drinking difficulties - drinking takes a long time, children fall asleep, there is no weight gain.
How is an atrioventricular septal defect (AVSD) treated?
Primary corrective surgery is usually performed between the 4th and 6th month of life. A diagnostic cardiac catheterisation is not usually necessary and is only performed if the diagnosis is made late or the anatomy is complex.
During the operation, the septal defects are closed with a patch and the AV valves are reconstructed. The prerequisite is that both chambers are the same size and the pulmonary pressure is not already too high.
If one chamber is too small, corrective surgery is not possible. In this case, the step-by-step procedure is the same as for complex heart defects with only one chamber (single ventricle) (see complex heart defects).
Reconstruction of the AV valves in AVSD is a high surgical skill. Minor leaks in the valve are common and only if these increase in the course of the disease must a valve reconstruction be attempted again after a few years.
In AVSD, the outlet from the left main chamber is shaped like a swan neck (goose neck); despite successful surgery, it can narrow in infancy and must then be widened surgically.